1
2
3
4
5
6
7
Diagnosis of AVN needs a comprehensive approach involving clinical inputs and radiological findings.
A doctor examines the patient thoroughly and checks for tenderness in joints. He might move joints through a variety of positions to check patient’s range of motion. In addition to the physical examination, understanding patient’s age along with detailed history is equally important. Occurrence of serious diseases in the past or previous medications may provide some diagnostic clues.


In 1969, Dr William H.Harris developed a hip scoring system which is currently being used by orthopedic surgeons all over the world.
Higher the score, the better. Low score indicates urgent need of doctor consultation.
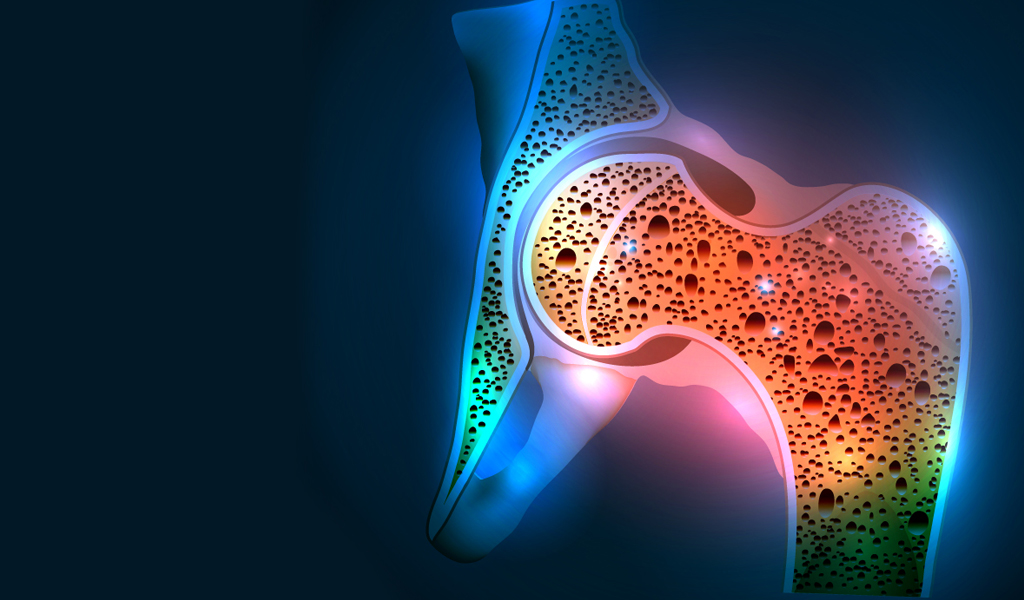
Obtaining image of bone is crucial for diagnosis of AVN. Usually a patient is asked to undergo a simple X-ray image of the joint.
Magnetic Resonance Imaging (MRI) is recommended for early stage from the disease onset. It is the most sensitive and specific method of Diagnosing AVN. It has the ability to detect the disease as early as 5 days after initiation of necrosis!
Radiological findings are essential to determine the Stage of disease and quantity of bone death.

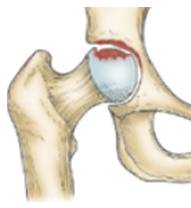
Stage of the disease gives idea about the progress of the disease. It simply means how much of the bone area is dead.. Various systems are being used for disease staging however, a system formulated by the Association Research Circulation Osseous (ARCO) is widely used in clinical practice.2
| How your bone looks | 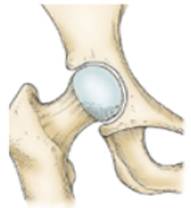 |
 |
 |
 |
| Symptoms | No symptoms | Mild symptoms | Severe pain and restricted movements | Severe pain and inability to move the joint |
| What does imaging test say? | Normal X-ray but abnormal MRI | X-ray shows presence of dead tissue even if the head of femur (thigh bone) appears normal in shape | Flattening of head of femur is observed and also fractures in the bone. If flattening of femur head is ≤2mm, it is stage IIIA. But if it is > 2mm it is stage IIIB. Additionally loosening of the cartilage is seen. | Joint destruction is seen with narrowing of joint space. Increased deterioration of bone tissue is seen on MRI. Cartilage is completely destroyed. |
| Stage | I II | III | IV | |
| Treatment Options |
|
|
|
|